Learn the common causes, prevention methods, and treatment options for pressure sores. Pressure sores commonly affect people with SCI due to paralysis and sensory loss.
Severe pressure sores can cause long-term damage, autonomic dysreflexia, and sepsis, which can be fatal.
On this pageDownload a printable PDF version of the SCI Wheelchair Usage Statistics Infographic or a PNG image to share online.
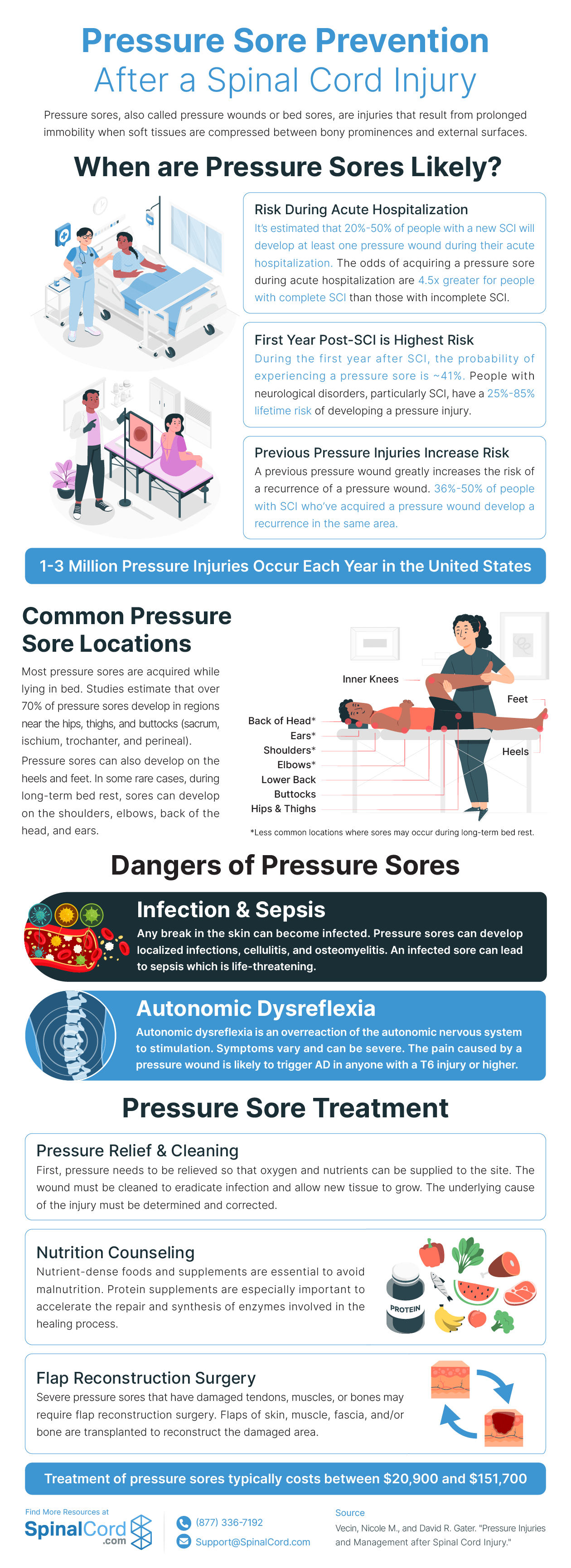
Pressure sores, also known as pressure ulcers, bedsores, or skin breakdowns, are injuries that occur when soft tissues are compressed between hard surfaces for a long time. The pressure reduces blood flow to these tissues, depriving the cells of necessary oxygen and nutrients resulting in tissue damage.
Pressure sores can cause pain, infection, sepsis, autonomic dysreflexia (AD), and spasticity. Complications caused by severe pressure sores can be fatal, so it's important to prevent pressure sores and treat them as soon as possible if they do occur.
Pressure sores are a common secondary complication of spinal cord injury due to paralysis, sensory loss, low blood pressure, and other risk factors associated with SCI.
1-3 Million pressure injuries occur each year in the united states.You are more likely to get pressure sores during your acute hospitalization after SCI. This is because you may spend a lot of time in bed, which can apply constant pressure on certain areas of your body.
Studies estimate that 20%-50% of people with a new SCI develop at least one pressure sore during their hospital stay. The risk is 4.5 times higher for people with complete SCI (no sensation or movement below the injury level) than those with incomplete SCI.
Your risk of getting pressure sores remains high during your first year after SCI, while you're adjusting to your new lifestyle and routines. You may also face challenges such as finding accessible housing, transportation, and equipment.
About 41% of people with SCI experience a pressure sore during their first year after SCI. The risk is higher for people who are older, have higher injury levels, or have other medical conditions that affect mobility or circulation.
If you have had a pressure sore before, you are more likely to get another one in the same area or somewhere else on your body. This is because the previous sore may have weakened your skin and tissues, making them more vulnerable to damage. You may also have habits or behaviors that increase your risk, such as not changing your position often enough or not checking your skin regularly.
According to some studies, 36%-50% of people with SCI who have had a pressure sore develop another one in the same area. The risk is higher for people who have larger or deeper sores, or who do not follow proper treatment and prevention guidelines.
Pressure sores are most likely to develop on bony prominences (parts of the body that have less padding from muscle or fat and that lie over a bone). The most common locations are parts of the body that are under pressure while sitting or lying down, typically in bed or in a wheelchair.
The most common locations where pressure sores develop:
During long-term bed rest, pressure sores may occur on the:
Pressure sores can cause serious complications that are potentially fatal including autonomic dysreflexia and sepsis.
Autonomic dysreflexia (AD) occurs when something below the injury level stimulates your nervous system. AD causes a sudden increase in blood pressure and heart rate. This can lead to headaches, sweating, flushing, nausea, blurred vision, and even stroke.
The pain or infection from a pressure sore can trigger AD in people with SCI at or above T6. If you have AD symptoms, you should seek medical attention right away.
Infection is when bacteria or other germs enter your body through a wound or sore and cause inflammation and pus. Sepsis is when an infection spreads throughout your bloodstream and causes organ failure and shock.
Pressure sores can become infected if they are not cleaned and treated properly. Infection can make your sore worse and harder to heal. It can also spread to other parts of your body through your blood vessels or bones. This can cause serious problems such as osteomyelitis (bone infection), cellulitis (skin infection), abscesses (pockets of pus), gangrene (tissue death), amputation (removal of a limb), sepsis, and death.
Pressure sores can delay your recovery and rehabilitation after SCI because they may:
The best way to prevent pressure sores is to avoid prolonged pressure on any part of your body. You can do this by:
If you notice any signs of a pressure sore on your skin, you should:
Download the infographic to print (PDF) or to share online (PNG).
SpinalCord.com. Pressure Sores After a Spinal Cord Injury, 6 Tips to Combat Pressure Sores After a Spinal Injury.
Vecin, Nicole M., and David R. Gater. Pressure Injuries and Management after Spinal Cord Injury. Journal of Personalized Medicine, vol. 12, no. 7, 2022, p. 1130.
Kruger, Erwin A., et al. Comprehensive Management of Pressure Ulcers in Spinal Cord Injury: Current Concepts and Future Trends. The Journal of Spinal Cord Medicine, vol. 36, no. 6, 2013, pp. 572--585.
{kind=link}